
Making decisions about induction of labour
This toolkit is to support you with choices if you have been offered Induction of Labour (IOL).
It may help you to make informed decisions about your care, in partnership with midwives
and doctors. It’s important for you to understand and be involved in your care planning which
includes discussing the reasons you are offered or recommended an induction.
An induced labour is one that is started artificially (not by itself). Around 3-4 out of 10 women
are induced in the UK. It is your choice whether to have labour induced or not and using this
tool can help you decide and help you ask questions.
Why might I be offered an induction of labour?
This tool is focused on supporting women and birthing people whose pregnancies have
continued past their due date and have been uncomplicated which means:
▪ You and your baby are healthy and well
▪ You are planning to have a vaginal birth
▪ You are having one baby only and the baby is in a head down position.
This toolkit may still provide some useful information for you but may not be
accurate if you have had any complications or concerns in your pregnancy. Your
own risk may therefore be different. In these situations, it is important for you to
have information personalised to you and your situation.
What are the benefits of IOL?
For most women and birthing people with uncomplicated pregnancies labour
will usually start naturally. Up to 82.8% of people going into labour by 41
weeks and 99% by 42 weeks.
There is increasing evidence to suggest that pregnancies continuing beyond the
due date have:
• Increased likelihood of the baby needing admission to a neonatal intensive
care unit
• Increased likelihood of stillbirth (when a baby dies before it is born) and
neonatal death
This is related to the placenta not working as well and therefore these risks
gradually increase the further past your due date your pregnancy continues.
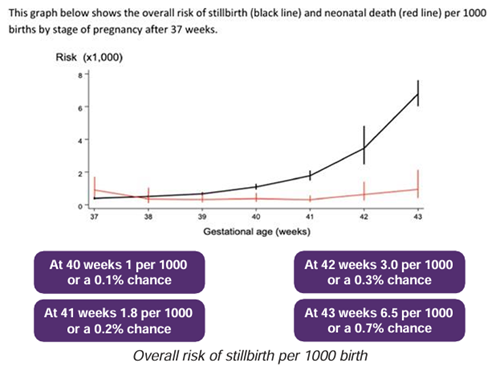
The information in a recent 2019 UK review of stillbirth rates from 15 million births from high
income countries is the one used most often as a guide (see information below).
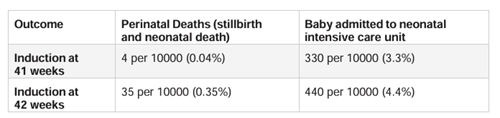
There is also national guidance that has looked at outcome from a much smaller amount of
women (less than 6000) who were induced at 41 weeks or 42 weeks. This also shows an
increase of perinatal death (both stillbirth and neonatal death) as pregnancy continued. 4 per
10000 for women having induction at 41 weeks; 35 per 10000 for women having induction at
42 weeks.
Although the chance of perinatal death is small overall there is no way of predicting whether
YOUR baby is at risk so the recommendation is to consider induction of labour at 41 weeks
to reduce the risks.
It is important that you think about the effect of induction on your birth experience when
making your choice and if you have any extra risks – speak to your midwife about these.
Pregnancy and birth past the due date are usually safe and straightforward for most
people and their babies, but sometimes problems can happen. Some problems are more
likely to happen depending on whether induction or continued pregnancy is chosen.
What are the risks of having an induction?
• The risks of choosing induction will vary depending on your own personal situation. It
may stop a serious infection occurring however it may affect your birth options and
limit your birth place choice.
• You may be recommended more interventions (for example, oxytocin infusion, vaginal
examination, continuous baby (fetal) heart rate monitoring and epidurals) which may
limit your ability to move around).
• There may be a need for an assisted vaginal birth (using forceps or ventouse), with
the associated increased chance of obstetric anal sphincter injury (OASI - third or
fourth-degree perineal tears). The OASI care bundle will be offered to try and reduce
this happening.
• There is a chance the medication used to induce labour could cause hyperstimulation – this is when the uterus (womb) contracts too frequently or contractions last too long.
This can lead to changes in the baby’s heart rate which could result in the baby being
compromised – we have clear guidelines to follow if there are too many contractions
and we monitor you to ensure your baby is coping with the contractions.
• You may be less likely to be able to use a birth pool.
• An induced labour may be more intense and painful than a natural labour as the
hormones don’t trigger the release of women’s own natural endorphins (which help
relieve pain)
• Your hospital stay may be longer than with a natural labour.
• Sometimes (1 in 100) induction of labour may be unsuccessful and other options
would be discussed with you and the midwives/doctors for a plan to be made together.
• Your highest chance of a vaginal birth is if it starts naturally (by itself) and you birth on
a Midwife-Led Unit near Delivery Suite.
Induction at 41 weeks
Women who chose to be induced at 41 weeks will be offered a membrane sweep prior to this
(see IOL leaflet) and given a date/time to attend Harmony Suite (based on our Delivery Suite)
for induction of labour.
We will try to book your IOL at 41 weeks if this is what
you have chosen. Sometimes we may need to make
changes to the date or time of your induction of labour
and a midwife will contact you if this happens. If you
are concerned about the date you have been given,
please speak to your midwife and she can look
into this further with the team.
Induction of labour can be a long experience.
Sometimes delays can happen. It is important
that a midwife is available to look after you in
the next stage of your induction. This is usually
when we break your waters. Our team will try to
keep you informed if any delays occur.
What are the Alternatives?
Continuing Pregnancy at 41 Weeks
Continuing pregnancy at 41 weeks means waiting for labour to start naturally.
You can choose to be induced any time from 41 weeks. We do not usually offer any extra
monitoring before 42 weeks if your pregnancy has been uncomplicated. Your midwife will
see you again at 41 weeks. She can offer you a membrane sweep.
If you have any additional risk factors your midwife will recommend further discussion with
the obstetric team or consultant midwife to make a personalised plan with you. This may
include extra monitoring. Extra monitoring cannot guarantee the wellbeing of your baby but it
may pick up concerns at the point of the monitoring.
It is very important to ensure your baby has a normal pattern of fetal movements and you
contact our Maternity Triage straight away if you experience a reduction reduced or change
in pattern of fetal movements. Please read your Fetal Movements Leaflet in your hand-held
records.
If you change your mind regarding any of your choices please contact the Maternity Triage
where a team member and take your details and you will be contacted.
Continuing Pregnancy at 42 weeks
Sometimes women choose to continue pregnancy beyond 42 weeks.
Although we offer extra monitoring for pregnancies over 42 weeks it is important for you to
know that this cannot identify all pregnancies which will be affected by stillbirth or death in
the newborn period. The chance of having a caesarean section increases after 42 weeks.
You will be recommended extra visits at the hospital to monitor the health of you and your
baby. Your midwife should refer you to a Consultant Midwife or Obstetric Doctor so you can
make a personalised plan with them.
What happens now?
• It is important to make a choice that is right for you.
• Try using the tool below to help you make a decision that is right for you and your baby.
• There is no rush in making a decision about whether to have an induction. You can go
home and think about it, read more, access our online Antenatal Education information on
the Wirral Women’s and Children’s Website or talk to your midwife or doctor again.
• If you choose to have an induction of labour, your midwife will arrange this and give
you further information.
• If you choose not to be induced you can change your mind at any
point.
• After 41 weeks the midwife will make a personalised plan with
you
• If you decide to continue pregnancy after 42 weeks, you
should be offered to see a consultant midwife or
consultant doctor to discuss your plans.
Think about...
What are the benefits?
What are the risks?
What are the alternatives?
What does your intuition or your gut feeling tell you?
What happens if we do nothing for now? Can we wait and take some time to think?
Second opinion...do I need one?
Further information
The Induction of Labour Information for
Birthing People and their families which
gives further information on induction of
labour
• including
• process
• risks
• membrane
sweep
• stages of
induction